CPR Resource Center
The most comprehensive library of emergency training resources — including videos, articles, downloads, and more.
The most comprehensive library of emergency training resources — including videos, articles, downloads, and more.
Transcutaneous pacing is a treatment option for symptomatic bradycardias unresponsive to Atropine or when Atropine is not immediately available. Additional indications of transcutaneous pacing include symptomatic bradycardia, most commonly resulting from acute MI, sinus node dysfunction, and complete heart blocks. Pacing is also recommended for severely symptomatic patients, especially when the block is at or below the His-Purkinje level (ie, type II second-degree or third-degree AV block).
Transcutaneous pacing can be extremely effective and is fairly quick to employ but due to the complexity of the devices it can be quite intimidating to use and learning barriers prevent rapid employment of this critical life saving tool. A study conducted in 2018 determined that out of two separate cohorts one comprised of 53 and 51 respectively, only 36% (18 participants) demonstrated they could effectively employ all 6 tasks during the study related to establishing effective transcutaneous pacing.
Flail chest
Bradycardia in the setting of severe hypothermia
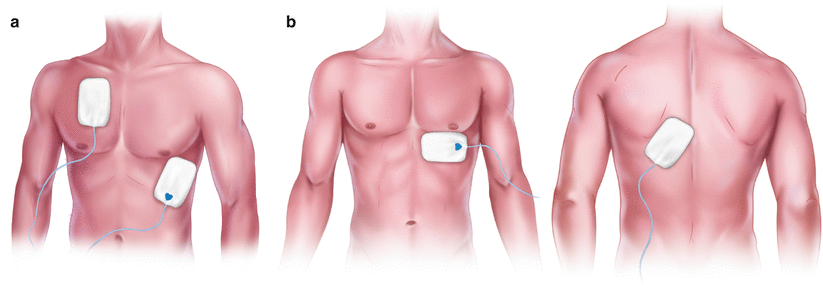
Transcutaneous pacing involves attaching two pacing electrodes on the patient’s skin placed in an anterior/ posterior approach (Figure B) The anterior (negative) electrode is placed o to the left of the sternum, halfway between the xyphoid process and left nipple. The posterior (positive) electrode is place in the left posterior thorax directly behind the anterior electrode. The pads can also be placed in an anterior/lateral approach (figure A).
A few key points to address for proper placement include ensuring the pads fit completely on the patient’s chest, have a minimum of 1-2 inches of space between electrodes and ensure no overlap or is that the electrodes are not placed on bony prominences of the sternum, spine, or scapula. Additionally, if defibrillation is necessary with paddles, place the defibrillation paddles about 2-3 cm (3/4 – 1 in) away from the pacer electrodes to prevent arcing.
Begin Transcutaneous pacing by connecting the patient to an ECG monitor to obtain a rhythm strip and confirm there is a rhythm which requires pacing. After placement of the pacing electrodes, connect the pacing cable to the electrodes and power on the device and set to “Pace” mode. Next you will want to set the pacing rate. Normally, the rate is set at a nonbradycardic rate between 60 and 80 beats per min. Next the output or milliamperes needs to be adjusted and set. You will increase the current slow and steady until electrical capture is achieved which is represented by a wide QRS and broad T wave.
Mechanical capture can be assessed by checking the pulses on the patient’s right upper extremity or right femoral pulse. Once electrical capture is achieved, adjust the pacing output or milliamperes just slightly above the level in which electrical capture was achieved. Generally, about 2 milliamperes above the initial electrical capture is sufficient. Effective pacing should produce an increase in blood pressure and level of consciousness but the patient should be monitored closely as the pacemaker can malfunction.
| Output (mA) | Patient Response |
| 20 | Prickly sensation on skin |
| 30 | Slight thump on chest |
| 40 | Definite thump on chest |
| 50 | Coughing |
| 60 | Diaphragm pacing and coughing |
| 70 | Coughing and knocking on chest |
| 80 | More uncomfortable than 70 mA |
| 90 | Strong, painful knock on chest |
| 100 | Leaves bed because of severe pain |
As you can see in the chart above, transcutaneous pacing can be painful especially as the output is increased. Most patients cannot tolerate currents of 50 milliamps and higher without sedation. Often times 50-100 mA are required for adequate pacing and the Ideal current is 1.25x what was required for capture. In a truly unstable patient, it is not uncommon for the patient to be hypotensive.
Sedation medications such as Benzodiazepines, Opioids or Propofol can have a negative effect on blood pressure so it is not uncommon for healthcare providers to also consider the administration of Epinephrine or Dopamine infusions in conjunction with sedation to prepare for transcutaneous pacing.
Transcutaneous pacing is a temporary solution for bradyarrhythmias. As such it is important to identify the contributing causes. An easy way to think of some of these causes are what we call the H’s & T’s.
Outside of the H’s & T’s, expert consultation should be considered when resulting to the use of transcutaneous pacing. There may very well be an electrical problem such as high-degree blocks in which conventional transcutaneous pacing may be ineffective. Issues such as inconsistent capture can take place Bradyarrythmias that are unresponsive to pharmacotherapy and transcutaneous pacing may require more advanced treatment to include transvenous pacing so it is imperative to seek expert consultation as soon as possible.
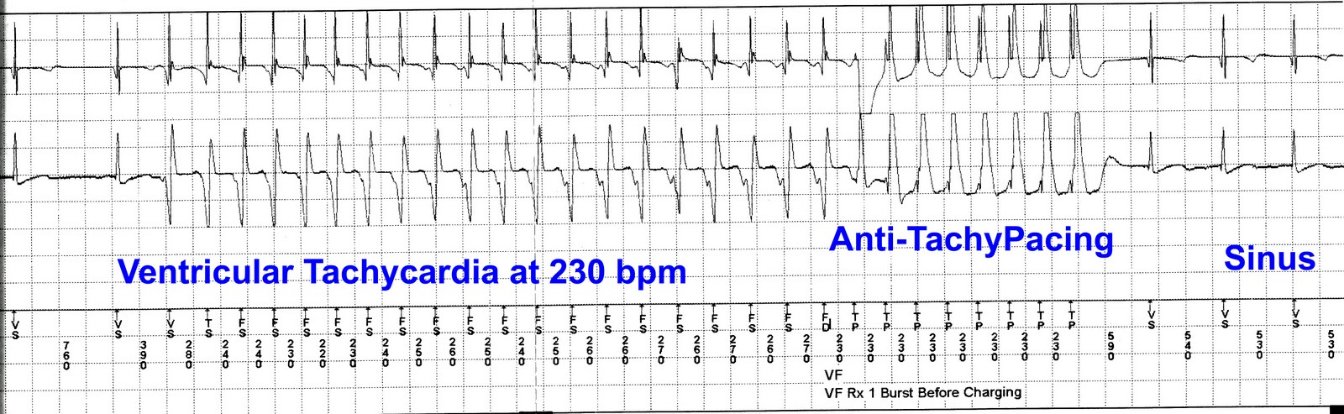
It may seem like a crazy idea but its not uncommon to use a form of pacing to override a native tachydysrhythmia. Overdive pacing, also known as anti-tachycardia pacing (ATP), attempts to correct the pathophysiology in supraventricular tachydysrhythmias but disrupting the reentrant circuit or over-riding the ectopic pacemaker with an external electrical impulse at a rate of 10 to 20 BPM greater than the native rate which changes the pattern of repolarization.
In refractory monomorphic ventricular tachycardia, ATP prevents abnormal ventricular automaticity by changing the pattern of ventricular depolarization and creating more uniform repolarization. In refractory polymorphic ventricular tachycardia, increasing the rate of ventricular depolarization decreases the ventricular refractory period, thereby reducing susceptibility to the R on T phenomenon.
Failure to capture is the inability of the pacemaker stimulus to depolarize the myocardium and is recognized on the ECG as visible pacemaker spikes not accompanied by P waves if the electrode is located in the atrium or QRS complexes if electrode is located in the right ventricle. Signs and symptoms of failure to capture can include fatigue, bradycardia, and hypotension. Failure to capture can be a result of battery failure, issues with pacing lead wires such as displacement, perforation of the myocardium, low energy output (mA) and much more. Low energy output is the most common cause so assessment of your patients is critical.

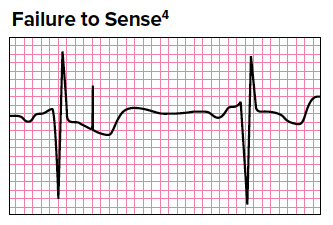
Failure to sense occurs when the pacemaker fails to recognize spontaneous myocardial depolarization. This malfunction is indicated on the ECG by pacemaker spikes that follow too closely behind the QRS complexes. This may result in pacemaker spikes falling on T waves which is known as the R-on-T phenomenon. The patient may complain of palpitations or skipped beats but this R-on-T phenomenon is much more serious and could precipitate ventricular tachycardia or ventricular fibrillation. Causes include battery failure, fracture of pacing wire, displacement of the electrode tip, antiarrhythmic medications and severe electrolyte imbalances.
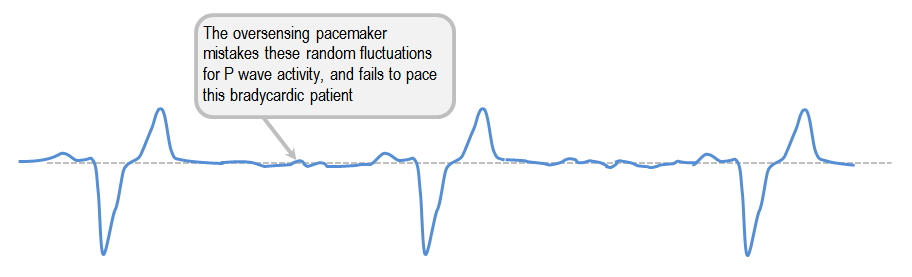
Oversensing is a pacemaker malfunction that results from inappropriate sensing of electrical signals. For example, atrial sensing pacemakers may inappropriately sense ventricular activity and ventricular sensing pacemakers may misinterpret a tall peaked T wave as a QRS complex. On an ECG, oversensing appears as pacemaker spikes at a rate slower than the pacemakers set rate (paced QRS complexes that come later than the pacemaker’s escape interval) or no paced beats even through the pacemaker’s rate is greater than the patient’s intrinsic rate. Treatment usually includes adjustment of the pacemaker’s sensitivity settings.
While Atropine may be the go-to medication for symptomatic bradycardia, not all patients respond to Atropine. It is important to have an alternative treatment at the ready for patients who do not respond to Atropine. Transcutaneous pacing is an excellent option for symptomatic bradycardic patients especially with certain AV blocks or long pauses. It is important that you are familiar with the equipment and follow your healthcare facilities protocols on who may be authorized to initiate this therapy.
To learn more about ACLS and PALS check out our BEACON Courses
Aehlert, B. (2006). ECGs made easy. St. Louis, MO: Elsevier Mosby.
Self M, Tainter CR. Overdrive Pacing. [Updated 2021 Jul 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK549874/
Tintinalli J, Stapczynski J, Ma OJ, Cline D, Cydulka R, Meckler G. Tintinalli’s Emergency Medicine, 7th ed., New York, NY: McGraw Hill Professional; 2010: Ch. 35
Help Me Find a Course